noso
ommeta
phobia.
An interactive explorer for posterior eye diseases

Case study
Hello!! Welcome to the Posterior Disease section, based on OPTM3205's content. Unfortunately the case-study generator is not online yet, and the first couple lectures have not yet been complete.
It will be ready as soon as possible.
Posterior Eye diseases
Number of Diseases so far
99

Systemic
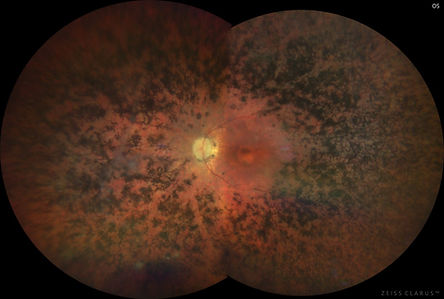
Diabetic Retinopathy
A systemic condition caused by diabetes which begins to impact the eye.
- Diabetes typically indicated for 11+ mmol/L BSL at random, 7+ mmol/L BSL during fasting
- Is strongly indicated for a HbA1c > 7% on two different tests to allow for irreversible glucose binding
- Longer duration of diabetes increases risk of DR by 6% annually, with a high risk after 10 years
Dystrophy
Retinitis Pigmentosa
A largely AR (50-60%), inherited and genetically heterogenous rod-cone dystrophy, caused by over 100 damaged genes. It is largely non-syndromic (70-80%), and can be of AD (30-40%) aetiology or X-linked (5-15%).
Dystrophy
CSNB
Congenital stationary night blindness refers to the group of conditions characterised by defective rod function, which leads to:
- Abnormal dark adaptation curve
- Abnormal ERG
- Nyctalopia

Inherited
Choroideraemia
An X-linked recessive condition affecting the CHM gene affecting the choroid, outer retina and RPE. This leads to nyctalopia, VF constrictions and can also have subtle appearance changes on female carriers.

Inherited
Gyrate Atrophy
Gyrate Atrophy is a relatively super rare AR condition affects the RPE, outer retina, and choriocapillaris. It causes nyctalopia, progressive field loss and ultimately central vision loss.

Dystrophy
BCD
A rare corneoretinal dystrophy that leads to crystalline retinal deposits scattered on the retina. This has a very distinct crystalline appearance present also in the sub-epithelial and anterior stromal layers of the cornea.

Inherited
LCA
Leber's congenital amaurosis is a rare inherited condition that usually causes profound rod and cone photoreceptor dysfunction. It is the most severe form of retinal dystrophy, causing visual impairment before first year of age.

Macular
Stargardt's Dystrophy
The most common childhood macular dystrophy. Is characterised by yellow pisciform flecks in macula which extends into midperiphery. This may lead to macular atrophy, and loss of rod cone function, and ultimately impacting central vision.

Macular
BEST Vitelliform Dystrophy
The second most common macular dystrophy, and has a classic eggyolk macula, and has 5 stages.

Macular
Pattern Dystrophy
A group of conditions characterised by variable distribution or pigment depositions at the level of the RPE.

Macular
Cone Cell Dystrophy
A dystrophy which targets the cone photoreceptors of the macula. Can cause poor VA, decreased colour vision or dyschromatopsia, and photophobia.

Macular
AD Drusen and X-Retinoschisis
Familial Dominant Drusen creates a number of drusen which is either radial, mosaic or honeycomb.
X-linked Retinoschisis causes the retinal degeneration and splitting of retinal layers with a spoke like macular appearance.

Optic Nerve Atrophy
LHON
Leber's Hereditary Optic Neuropathy is a congenital swelling of the optic nerve axons causing nerve fibre death, colour vision loss, thinning of the fovea, and central/ceco-central scotomas

Optic Nerve Atrophy
AD Optic Neuropathy (Atrophy)
AONA is caused by a damage in mitochondrial metabolism architecture, leading to dyschromatopsia, and ceco-central scotomas

Disc Excavation
Optic Disc Coloboma
Enlarged nerve head, due to incomplete closure of optic fissure, typically affecting the inferior/infero-nasal neuroretinal rim.

Disc Excavation
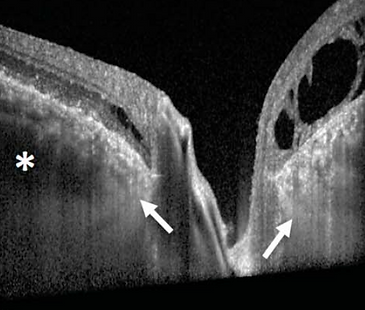
Congenital Optic Disc Pit
Classically seen as a lower temporal grey oval in the optic disc that rarely affects the visual acuity of a patient however, can lead to retinal schisis and maculopathy

Disc Excavation
Morning Glory Syndrome
Characterised by a shape similar to the morning glory flower due to radial spoke like blood vessels which emerge, as well as the pale centre matching the flower, which is due to white glial tuft. May have chorioretinal pigment hyperpigmentation around the disc.

Disc Excavation
Megalopapilla
An abnormally large optic disc, with an area greater than 2.5mm^2

Developmental
Chorioretinal Coloboma
Caused by the failure of the choroidal fissure to close on day 44, leading to the failed formation of ocular tissue. Whilst it affects the iris, lens, choroid, retina and optic nerve, chorioretinal coloboma affects only the choroid and retina, though can be associated with other colobomas.

Developmental
ROP
Retinopathy of Prematurity is a retinal disease associated with the improper development of retinal BV, most commonly in premature infants and low birthweight infants.

Acquired
TIA
A binocular or monocular temporary loss of vision that can be easily missed due to visual input from the non-affected eye compensating for the missing signal. Transient vision loss is only referred to as TIA if neurological dysfunction is caused by a focal brain, spinal cord or retinal ischaemia without infarction.
This means it is not a stroke.

Acquired
Retinal Vein Occlusion
Comes in many forms. It can be either branched or central, of the acute or chronic form.

Acquired
Retinal Artery Occlusion
Comes in many forms. It can be either branched or central, of the acute or chronic form.

Inherited
Sickle Cell Retinopathy
Due to sickle cell gene mutation, causing breakdown of blood at a faster rate. This causes anemia and jaundice. Leads to RPE hypertrophy and sea-fan neovascularisation.

Acquired
Eales' Disease
An idiopathic inflammation of the peripheral retinal veins, leading to periphlebitis.

Acquired
Ocular Ischaemic Syndrome
Occurs with a stenosis of the internal carotid artery, leading to ocular hypoperfusion and ischaemia. Consequently also affects the eyes, leading to iris neovascularisation, and painful neovascular glaucoma.

Systemic
Arteritic AION
A systemic inflammatory condition leading to severe acute vision loss, visual field defects, and is generally irreversible. Is considered an ocular emergency, and requires emergency attention immediately.

Acquired
Non-Arteritic AION (NAAION)
As implied, occurs due to the blockage of the short posterior ciliary arteries, without inflammation of the arteries, and primarily affects the optic disc. Is typically less severe than AAION.

Acquired
Pachychoroid Pigment Epitheliopathy (PPE)
The first stage of pachychoroid syndrome, occuring when the RPE is able to withstand increasing fluid pressure from the hyperpermeable choroid, by actively pumping fluid back out.

Acquired
Central Serous Chorioretinopathy (CSCR)
Occurs when the RPE cannot overcome the pressure of the hyperpermeable choroid, leading to outer blood retinal barrier breakdown.

Acquired
Pachychoroid Neovasculopathy (PNV)
Occurs following damage to the Bruch's membrane, and outer retinal ischaemia. Angiogenesis begins due to VEGF release, leading to T1 NV.

Acquired
Polypoidal Choroidal Vasculopathy (PCV)
The development of aneurysmal lesions in PNV lead to the development of PCV, characterised by steep peaked PEDs

Acquired
Focal Choroidal Excavation (FCE)
Characterised by excavation of choroidal tissue without scleral abnormalities, without affecting the overlying retina. Can be conforming or non-conforming
Acquired
Peripapillary Pachychoroid Syndrome
Pachychoroid occurring next to the optic disc, with classic thickening

Telangiectasia
Coat's Disease
A progressive disease characterised by retinal telangiectasia.

Telangiectasia
MacTel 2
Macular Telangiectasia 2 is actually a neurodegenerative condition, with the possibility of accompanying telangiectasia.

Systemic
Hypertensive Retinopathy
Retinopathy caused by increased blood pressure in the body system due to numerous factors, which leads to both chronic and acute changes to the vessels, and exudative deposits.

Systemic
Hypertensive Choroidopathy
A systemic condition typically seen with hypertensive retinopathy affecting the choroid. Typically seen in younger patients with an acute increase in BP with systolic pressure > 180mmHg

Optic Nerve Atrophy
Primary Optic Disc Atrophy
Describes a large range of conditions all characterised by the death of axonal cells without optic disc swelling preceding it. It's most common presentation is typically optic neuritis, but can present from other aetiologies.

Optic Nerve Atrophy
Secondary Optic Atrophy
Axonal damage preceded with the longstanding swelling of the optic nerve. Chronic oedema can impinge and damage nerve fibres, leading to marked degeneration, and cause profuse glial tissue proliferation.

Optic Nerve Atrophy
Consecutive Optic Atrophy
Associated with diseases affecting the inner retina or blood supply, and in an anterograde fashion, the retinal axons to then impact the optic nerve tissue.

Optic Nerve Atrophy
Retrograde Optic Atrophy
Damage to the brain or visual pathway that progresses to the retina, leading to damage and atrophy there.

Glaucoma
Primary Open Angle Glaucoma
A group of ocular disorders of multi-factorial aetiology, united by a clinically characteristic optic neuropathy with potentially progressive clinically visible changes at the ONH, comprising focal or generalised thinning of the neuroretinal rim with excavation and enlargement of the optic cup, representing neurodegeneration of the of the retinal ganglion cell axons and deformation of the lamina cribrosa. Corresponding diffuse and localised nerve-fibre-bundle pattern visual field loss may not be detectable in early stages; while VA is initially spared, progression can lead to a full loss.

Glaucoma
Secondary Open Angle Glaucoma
SOAG is an open angle glaucoma that has a identifiable aetiology behind the increase in IOP, despite an open angle. Typically due to obstruction of the angle due to pigments, particles, etc.

Glaucoma
Angle Closure Glaucoma
PACG and SACG are a collection of glaucomas characteristed by elevated IOP, following anatomical iridotrabecular contact, or in the case of SACG, due to a pathological mechanism other than anatomical.
Posterior Tumours
Iris/Ciliary Tumour Overview
Due to the partly anterior nature of uveal tumours, this slide serves just as a basic overview for some of the more common iris and ciliary body tumours.

Posterior Tumours
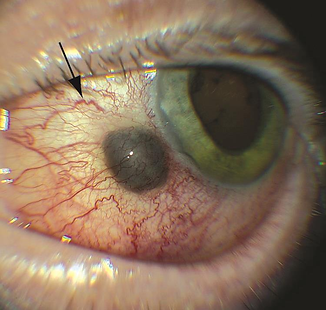
Choroidal Naevus
A benign melanocytic lesion that presents on the choroid, however, has a risk of developing into a malignant melanoma.
Has a dark and light manifest, and is typically asymptomatic.

Posterior Tumours
Choroidal Melanoma
Choroidal melanoma is a rare cancer that develops in the choroid and pushes inwards. It develops from melanocytes, and possibly from choroidal naevi

Posterior Tumours
Optic Nerve Melanocytoma
A melanocytoma is a rare benign lesion located in the optic nerve head, choroid, iris, ciliary body or diffusely in the uvea, conjunctiva or sclera. The ON melanocytoma is thus specifically at the optic nerve, and contains melanocyte sand myelin. This can then extend into the RNFL

Posterior Tumours
Choroidal Haemangioma
Very rare benign vascular tumours, composed of vessels. Usually dome shaped with a red-orange mass, commonly at the posterior pole.

Posterior Tumours
Choroidal Osteoma
A rare benign slow-growing bony tumour

Posterior Tumours
Posterior Eye Metastasis
Is not a disease itself, but rather describes the theories of ocular metastasis, or when a cancer in the body migrates to the eye to further develop and cause secondary cancer. Overall it is a very rare condition, and typically undetected until after death.

Posterior Tumours
CHRPE
Congenital Hypertrophy of the Retinal Pigment Epithelium. A benign pigmented lesion that is usually asymptomatic.

Posterior Tumours
RPE Adenoma/Adenocarcinoma
Rare intraocular tumours that are very similar to choroidal melanomas, uveal melanomas, CHRPE and others. It is important to recognise that whilst the adenoma is benign, adenocarcinoma is malignant.

Posterior Tumours
Retinal Astrocytoma
Otherwise known as retinal astrocytic hamartoma are benign glial cell tumours that are usually asymptomatic.

Posterior Tumours
Retinoblastoma
Otherwise known as Rb, it is a very rare cancer that develops in the retina, primarily affecting children and diagnosed before the age of 5. Whilst treatment is very effective, if left untreated is fatal. Urgent referrals are always necessary

Intraocular Lymphoma
PVRL
Primary Vitreoretinal Lymphoma is one of the 3 types of intraocular lymphoma. It is a high grade lymphoma that affects the vitreous body, retina and the optic nerve. These are typically composed of large B-cell lymphomas. VRLs can be secondary, known as DLBCL, or CNS involving or PCNSL.

Intraocular Lymphoma
Choroidal Lymphoma
Choroidal lymphomas are a subset of uveal lymphomas, which are primary low grade B-cell lymphomas. Choroidal lymphomas can also include intraocular involved secondary/systemic lymphomas.

Orbital Tumours
Capillary/Cavernous Haemangioma
A benign orbital tumour involving the capillary system

Orbital Tumours
Optic Nerve Glioma
A benign tumour consisting of astrocytes and glial cells that slowly grows from the optic nerve, chiasm or tract.

Orbital Tumours
Orbital Lymphoma
Tumours that arise from germinal central cells or memory B cells which have undergone antigen exposure. Can also be from T-cells

Orbital Tumours
RMS
Rhabdomyosarcoma is a tumour that arises from the connective tissues of the eye, such as muscle, fat, bones and blood vessels, hence the name sarcoma.

Orbital Tumours
Orbital Meningioma
Slow growing benign tumours which arise from the optic nerve sheath, specifically from the arachnoid cells.

Orbital Tumours
Lacrimal Gland Tumours
Rare epithelial and non-epithelial lesions. Involves both benign tumours such as pleomorphic adenoma, and myoepithelioma, as well as malignant tumours such as adenoid cystic carcinoma.

Orbital Tumours
Sinus Invasion Tumours
A tumour from the sinus that invades the orbit. Early detection is critical considering the conditions poor prognosis

Orbital Tumours
Neuroblastoma Orbital Metastasis
Neuroblastoma cells which have metastasised to the orbit, typically from breast or lung cancer

Neurocutaneous Tumours
Neurofibromatosis
Tumorous growth on nerve tissues that can affect the eye. Typically is a genetic condition.

Neurocutaneous Tumours
Tuberous Sclerosis Complex
A genetic multisystem disorder causing widespread hamartomas in organs such as the brain, heart, skin, eyes, kidney, lung and liver. In the eyes, it is responsible for retinal hamartomas, such as the retinal astrocytoma.

Neurocutaneous Tumours
von-Hippel-Lindau Syndrome
A benign retinal capillary haemangioma in the retina with associated dilated feeder vessels that are typically isolated

Neurocutaneous Tumours
Sturge-Weber Syndrome
A rare congenital sporadic condition that affects the face, eyes, leptomeninges and is accompanied by vascular hamartomas.

Acquired
Age Related Macular Degeneration
AMD is one of the leading causes of vision loss worldwide, and describes the age related changes of the eye and its progressive degeneration.

Macular
Myopic Maculopathy
A pathological extension of high myopia, leading to atrophic, tractional and neovascular changes. Whilst high myopia is not pathological, myopic maculopathy involves

Vitreomacular
Normal Vitreous Changes
Some changes to the vitreous, and vitreomacular interface is normal, and often age related. This section aims to explore these changes to differentiate from abnormal changes.

Vitreomacular
Vitreomacular Adhesion and Traction
Describes two conditions. The first is the persistent adhesion of the vitreous to the macula, and the second is the tractional force the vitreous may exert on the macular.

Vitreomacular
Macula Pseudohole and FTMH
A pseudohole is not a true hole, and in most cases, are simply holes which appear as cavities with a break in the surface. On the other hand, a true hole is one that spans the full thickeness of the macula.

Vitreomacular
Epiretinal Membranes
A common finding that is present in numerous diseases, such as retinitis pigmentosa, coat's disease, neurofibromatosis 2, macular pseudoholes due to schisis, uveitis.

Peripheral Retina
Non-vision Threatening Peripheral Retinal Degenerations
Describes the category of retinal degeneration that is generally unharmful, and will not progress to affect central vision.

Peripheral Retina
Retinal Holes
The first set of potentially vision threatening peripheral retinal lesions. Consists of the atrophic retinal holes and operculated retinal holes.

Peripheral Retina
Horseshoe Retinal Tear
Is a specific type of vision threatening retinal break. This typically arises in the superior fundus, where it can then expand downwards to affect central vision.

Peripheral Retina
Lattice Retinal Degeneration
Apart of the category of abnormal vitreoretinal attachments, as neither a break nor a hole. Includes lattice degenerations and snail track degenerations.

Peripheral Retina
Vitreoretinal Anomalies and Tufts
Includes the snowflake degeneration, non-cystic and cystic vitreoretinal tufts.

Peripheral Retina
Retinoschisis
Retinoschisis describes the neurosensory splitting of the retina, and is a common differential from RRD. Only 1.6% leads to RRD, requiring both inner and outer schisis.

Traumatic
Closed Globe Injuries
Closed globe injuries are injuries which can occur without any entrances into the eye. This is commonly due to injuried such as blunt trauma.

Traumatic
Open Globe Injuries
A form of injury where the sclera or cornea is breached, causing a full thickness wound in the eyeball, and this can lead to inflammation and damage at different parts of the eye.

Traumatic
Orbital Trauma
Covers the trauma in very brief recap of the content previously explored in the anterior eye segment

Inflammatory
Sarcoidosis Uveitis
Is the manifestation of sarcoidosis in the eye. The infection triggers granulomas in multiple tissues, such as the lungs and eyes.

Inflammatory
VKH Syndrome
Vogt-Koyonagi-Harada syndrome is a condition previously explored in the anterior eye disease segment. Is a rare autoimmune condition primarily affecting melanin rich tissues.

Inflammatory
SLE Uveitis
Systemic Lupus Erythematosus is an autoimmune condition affecting the connective tissues and can have various ocular manifestations, namely retinopathy, choroidopathy and neuro-ophthalmic conditions.

Infectious
Herpetic Uveitis
Whilst uveitis can be due to viral causes, and many viral causes such as HIV/AIDS, this section only concerns the herpetic family of viruses which causes posterior eye disease manifestations.

Infectious
Endogenous Endophthalmitis
Spread of bacteria or fungus from the blood from a remote infection site, which moves to the eye. Whilst can be due to bacteria or fungus, this section mainly focuses on bacterial.

Infectious
Syphilitic Chorioretinitis
Syphilis is a disease caused by treponema pallidum, leading to various systemic diseases. Uveitis was covered in the anterior segment, but it will briefly be explored again.

Infectious
Tuberculosis Retinitis
Caused by mycobacterium tuberculosis, leading to chronic progressive granulomatous infection commonly via hematogenous spread.

Infectious
Toxoplasmosis Chorioretinitis
Toxoplasmosis is caused by a parasite known as toxoplasma gondii

Infectious
Toxocariasis Uveitis
Caused by the nematode toxocara canis, and can have both systemic manifestations in the major organs, as well as ocular manifestations due to larvae migration.

White Dot Syndrome
MEWDS
Multifocal Evanescent White Dot Syndrome
Primary features: F > M, 20-50, mostly unilateral, acute, variable, 5 WDS symptoms, for weeks-months, rare, with myopia, small white dots in outer retina, disc oedema, mild vitreous cells, rare CNV, very good prognosis and no HLA.

White Dot Syndrome
APMPPE
Acute Posterior Multifocal Placoid Pigment Epitheliopathy
Typical features include, M = F, 20-30s, bilateral and acute onset, variable viral prodome, Classic WDS symtpoms, resolves in weeks-months, recurrence is rare, multifocal flat gray-white placoid lesions at the level of the posterior pole. RPE improving within 1-2 weeks, and can have disc swelling. Mild vitreous cells, no CNV, good prognosis but can have RPE mottling and depigmentation.

White Dot Syndrome
MFC and PIC
Will cover Multifocal Choroiditis and Punctate Inner Choroidopathy
PIC Features: F > M, affects <40years, bilateral, sudden onset, no viral prodome, decreased central VA and WDS. Rare recurrence. Small multiple gray/yellow/opaque round lesions at the level of the RPE-choroid, scattered throughout the posterior pole. Evolves usually into atrophic chorioretinal scars, may be complicated by CNV or subretinal fibrosis. No vitreous cells, 1/3 develop CNV, good prognosis, but scarring and CNV may occur.
MCP Features: F > M, affects 20-60s, bilateral, insidious onset, variable viral prodome, WDS symptoms, chronic duration, recurrency is common, myopic, iritis in 50%, yellow/white lesions whic are replaced by punched out scars. Moderate vitreouc cells, CME may be seen with CNV and generally poor prognosis.

White Dot Syndrome
Birdshot Chorioretinopathy
BSC features: primarily affects adult females. Bilateral, with insidious onset and no viral prodome. Classical WDS symptoms but with floaters and difficult night vision, colour vision. Chronic and recurrent. Multiple ill-defined cream lesions at level of outer retina/RPE. Patches of depigmentation, optic atrophy and some disc swelling. Moderate vitreous cells, CME and rare CNV. Guarded prognosis, and strong associateion with HLA-A29.

White Dot Syndrome
Serpiginous Choroidopathy
Predominantly affects males of 30-60s. Bilateral but asymmetrical, with variable onset and no viral prodome. Classical WDS symptoms, but with paracentral scotomas sometimes. Chronic, and recurrent acute lesions last weeks to months. Pseudopodial/geographic zones of gray-yellow discolouration of RPE in peripapillary and macular area with centrifugal extension. Active and peripheral edge at the RPE and choriocapillaris. Vitreous cells can be present or absent, CNV is rare, prognosis is gaurded. Can have RPE mottling, scarring, loss of choriocapillaris and CNV. Associated with HLA-B7, S-antigen.